
Insulin is crucial for the control of numerous metabolic processes and is essential for our bodies. Sadly, this important hormone has a very bad reputation being considered to be ‘fattening’. In general, it is true that insulin’s task consists in shifting metabolic processes towards energy storage and carbohydrate utilization. However, this does not mean that insulin makes a person fat. It is calorie overconsumption what causes weight gain.
The role of insulin1
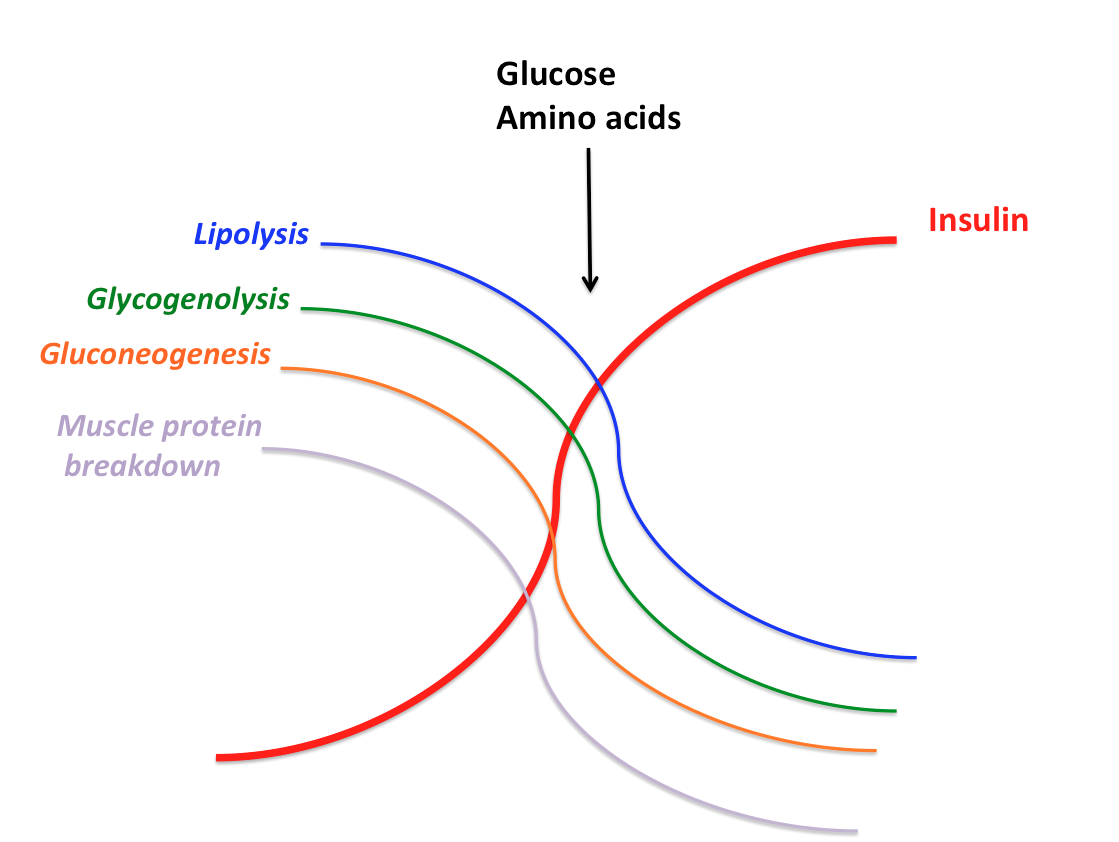
Insulin is a regulatory hormone that is secreted when we consume carbohydrate and/or protein-rich food. Insulin acts like a break by signaling the body that processes involved in release of stored energy have to be stopped and the consumed nutrients have to be stored.
In the fasted state - when we sleep for example - our bodies mobilize stored energy to support essential metabolic processes. Fatty acids are broken down and used to produce ketones to be utilized by various tissues as fuel. Liver glycogen (glucose storage) is broken down to maintain the required blood sugar level and support glucose-dependent processes in the brain and red blood cells. When liver glycogen decreases, our bodies start their own glucose production by using mostly amino acids as glucose building blocks. Muscle protein breakdown provided the required amino acids for glucose production.
After a meal, in the fed state, insulin levels rise and stop the described catabolic processes. Additionally, insulin facilitates nutrient uptake into the cells, for example by increasing the number of glucose transports on the cell surface. However, insulin is not necessarily required for glucose uptake.
What happens when insulin is lacking?1
The lack of insulin results in the absence of the described breaking mechanism. Such a condition occurs in diabetes type I. The breakdown of fat, glycogen and muscle tissue does not stop even in the fed state. The loss of control over these processes, leads to an steady increase in glucose and ketones in the blood stream. Uncontrolled ketone production causing abnormally high blood ketone levels decreases blood pH and can be fetal. However, this process, called ketoacidosis, should not be confused with controlled ketosis. Controlled ketosis occurs during long periods of fasting or on a ketogenic diet and is required to supply tissues with energy in form of ketones.
It is not only sugar that increases insulin
Although an increase in insulin levels is usually associated with sugar, it is important to note that essential amino acids, especially branched chain amino acids leucine, isoleucine and valine, lead to insulin secretion.2–4
Indeed, consumption of dairy products, such as milk and whey protein that are high in leucine, was shown to elevate insulin levels more than white bread despite lower measured blood glucose concentration overtime.5
Insulin promotes hunger and weight gain - truth or myth?
It is a wrong, widespread belief that insulin has ‘fattening’ prosperities. Actually, the opposite is the case. Insulin reduces appetite and food intake through its regulatory functions in the brain.6,7 In this context, it is likely that a drop in blood glucose levels and not necessarily the function of insulin results in hunger and increases food intake.8 Additional evidence provides the fact that high protein diet increases satiety despite spiking insulin levels.9
Bottom line
Insulin is demonized to be the bad hormone that makes us fat. Often, the success of low carb diets is justified with the argument that insulin levels are kept low. However, considering the fact that such diets are mostly high in protein the ‘low insulin argument’ does not apply, in my opinion. The success of low carb diets is mostly due to the satiating effect of protein and restricted food selection.
Insulin is NOT bad. This hormone is essential for our health and metabolic regulation. Although, insulin inhibits fat utilization in the fed state, it does not make us fat. Insulin levels start decreasing some time after a meal and are low when we sleep at night. That is when more fat is used as energy source. We should not obsess over hormonal response that occurs only for a limited time after a meal, but look at the entire 24-hour period. Here, it is balance between calorie expenditure what matters for body composition goals and not what happens after a single meal.
References:
(1) Sonksen, P.; Sonksen, J. Br. J. Anaesth.2000, 85, 69–79.
(2) Loon, L. J. C. Van; Saris, W. H. M.; Verhagen, H.; Wagenmakers, A. J. M. 2000, 96–105.
(3) Calbet, J. A. L.; Maclean, D. A. 2002, 2174–2182.
(4) Floyd, J. C.; Fajans, S. S.; Conn, J. W.; Knopf, R. F.; Rull, J. J. Clin. Invest.1966, 45, 1487–502.
(5) Nilsson, M.; Stenberg, M.; Frid, A. H.; Holst, J. J. Insulin2004, 1246–1253.
(6) Kleinridders, A.; Ferris, H. a.; Cai, W.; Kahn, C. R. Diabetes2014, 63, 2232–2243.
(7) Somogyi, V.; Gyorffy, a; Scalise, T. J.; Kiss, D. S.; Goszleth, G.; Bartha, T.; Frenyo, V. L.; Zsarnovszky, a Nutr. Res. Rev.2011, 24, 132–54.
(8) Chaput, J.-P.; Tremblay, a Int. J. Obes. (Lond).2009, 33, 46–53.
(9) Gerstein, D. E.; Woodward-Lopez, G.; Evans, A. E.; Kelsey, K.; Drewnowski, A. J. Am. Diet. Assoc.2004, 104, 1151–3.